A wide-ranging review of the past 60 years of clinical practice (i.e. Baldwin, Wampold & Imel, 2007) shows that the number one factor for therapeutic success is a high-quality alliance between therapist and client, and a clarity around the goals and tasks of therapy. In this article we will provide:
- a meta-conceptual framework explaining the spectrum of therapists’ influence over the course of therapy
- specific questions, stemming from humanistic sciences (Maslow & Rogers, 1979), which help clients be more empowered, build more autonomy and trust of their own capacity
Meta-conceptual framework of clinical interventions
The initial goal of therapy is to help the therapist gain the client’s trust to build a strong alliance and raise epistemic confidence (the clients’ confidence in themselves to find their own solutions). This involves a progressive development of intimacy and trust between the therapist and client, which can be realized with the following options of therapeutic possibilities (see Diagram 1).
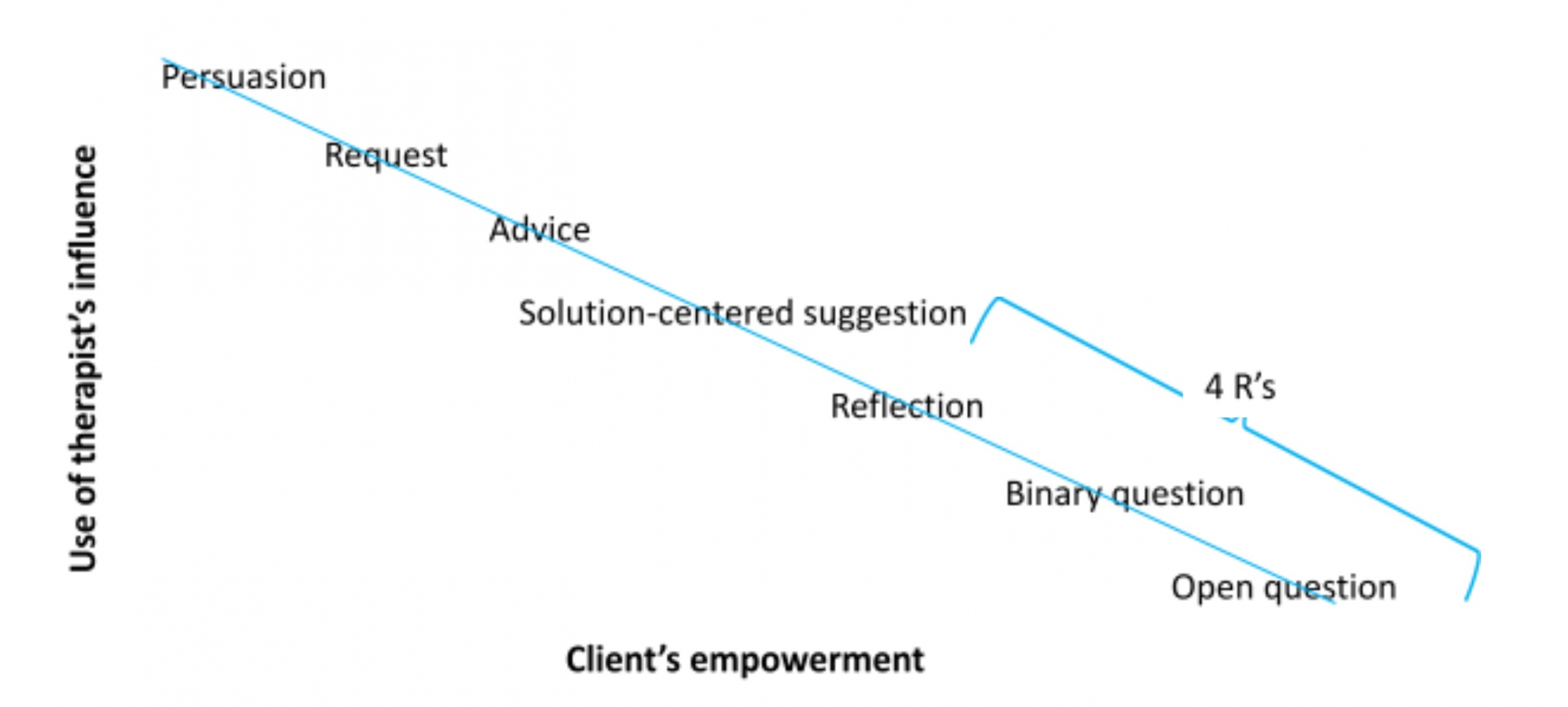
Diagram 1. Spectrum of therapeutic interventions as a client becomes more empowered.
Diagram 1 represents the spectrum of therapeutic interventions from more power-rich (though not power-over) to more empowering forms. This map is linear, and helpful to understand the overall journey of a client, with specific clinical interventions. However, it is important to note that as organisms, with our complex structure and non-linear cycles, we will need far more attunement and sensitivity than a simplistic formula such as this one to succeed in empowering our clients. Nevertheless, this may initially provide a helpful structure.
When a client is severely unwell, it will be helpful to provide a strong frame and use our suggestive authority to help strengthen their socio-emotional container. The interventions of persuasion (i.e. “you will need to take medication”), requests ( i.e. “please make sure you go for a walk in nature everyday”)and advice-giving (i.e. “I would recommend that you have some rest after our session”) will tend to fall in this category.
Solution oriented proposals will orient our clients strongly towards the positive, the constructive, the skilfull (i.e. “imagine you were able to achieve your goal, how would that be for you?”). It helps support a deeper sense of embodiment, confidence and belief in their agency and ability.
The 4 R’s follow: reformulate, recontextualize, review, and reinforce:
- Reformulate: using an impressionist form and tone, reflecting/mirroring back to the client what has been heard to show the therapist understands what they have shared and helps build/restore the therapist-client collaboration and dance. Reformulations also help structure the narrative and/or present emotion, key points can be amplified, emphasize the posture of curiosity and not-knowing, the therapist can also make helping additions and use different wordings to broaden the discourse, while checking the client shares these developments. In most reformulations, there is the formulation of a relatively complex hypothesis relevant to the client. These are sub-categories of reformulation:
- Simple repetition (parrot): reflect back word-for-word what the client shared, as precisely as possible (usually for high arousal disclosures).
- Verification: verifying the meaning of certain sentences, feelings, descriptions
- Simple reflections: neutral reformulation
- Double reflections: repeating two often contradictory points of view or experiences to underline ambivalence (refrain from using “but”)
- Recontextualise: help bring greater precision and specificity to the client’s situation (difficulty or ease). Asking for examples or situations that are space and time bound enables a crossover from a more conceptual, verbalized cognitive generality to an embedded and embodied experience. This promotes a re-centering of attention on the experiential qualities of the discourse/narrative and allows give opportunities for the client to feel recognized and understood by the therapist. Here are some examples:
- “Could you give me a recent example of what you are describing?”
- “When was the last time this occurred?”
- “How does this manifest in your daily life?”
- Review/Recap: summarise the client’s sharings to make sure they have been understood. They can occur at any time and may be very brief (2-3 sentences) or quite in-depth (a few minutes). Recapping helps the client feel understood and build a common vision and therapeutic alliance. They can be particularly useful at the end of a session to start slowing down and reducing new input into the session, as well as revisiting some of the key themes and moments of the session. The client participation can also be encouraged by asking them to review the session(s) themselves, saying for example:
- “What have been the key learnings/takeaways/experiences from this session?”
- “What do you make of all of this?”
- “In one word, how would you sum today’s exchange together?”
- Reinforce: positive reinforcement is part of a shaping and conditioning paradigm which aims at increasing the level of confidence in certain pattern, thereby raising the probability of that skillful behaviour to arise again. It is a powerful tool initially to strengthen the therapeutic alliance, and then supports the client’s feeling of self-efficacy. They offer important spaces for satisfaction, appreciation and celebration in the midst of the client recounting challenging situations. One can reinforce:
- Facts: underline a client’s action or behaviour in the past or in the present, which they have done or refrained from doing.
- People: emphasize the helpful qualities present as the client is sharing.
- Affect: recognizing suffering, normalizing it and offering encouragement and compassion (i.e. “in this situation, it is normal to feel…”)
May this article be for the benefit of all beings.
You can learn more about the application of these evolutionary and systemic models, their associated neuroscientific empirical research, practice and interventions along with time for practice in our workshops, courses and trainings at www.neurosystemics.org.
Together we go further.
References
Baldwin, S. A., Wampold, B. E., & Imel, Z. E. (2007). Untangling the alliance-outcome correlation: Exploring the relative importance of therapist and patient variability in the alliance. Journal of consulting and clinical psychology, 75(6), 842.
Maslow, A. H., & Rogers, C. (1979). Humanistic psychology. Journal of Humanistic Psychology, 19(3), 13-26.